|
|
Bisphosphonate-related Osteonecrosis of the Jaw
(BON) (BRONJ)
General Considerations
- Bisphosphonates are commonly prescribed for the treatment and prevention of
- Osteoporosis (e.g. alendronate, risendronate, ibandronate)
- Osteolytic lesions in metastatic bone tumors (e.g. breast, prostate, multiple myeloma) (e.g. zoledronate, pamidronate)
- Hypercalcemia associated with malignancy
- Bind and inhibit osteoclastic activity
- There has been an association described between bisphosphonates, usually in higher doses in cancer patients, and avascular necrosis, especially of the mandible
- Incidence has been most strongly correlated with pamidronate (Aredia) and zoledronic acid (Zometa)
- Many develop after tooth extraction which may serve as a trigger
- Latency of 5-36 months after therapy before osteonecrosis occurs
- More common with IV administration of drug than oral
Clinical Findings
- Exposed, non-vital bone
- Pain
- Swelling
- Trismus
Imaging Findings
- Confined to mandible (majority) and maxilla
- Mixed lytic and sclerotic lesion of the jaw
- Sequestration
- Pathologic fracture
- Periosteal reaction
- MRI-low T1 and T2 with exposed bone and low T1 and high T2 in unexposed bone
Differential Diagnosis
- Metastatic bone lesion
- Osteomyelitis
Treatment
- Difficult
- Discontinue bisphosphonate therapy
- Avoid dental extractions
- Medical therapy may include antibiotics used locally and systemically
- Surgical curettage has been used
- Chemical debridement with antiseptic irrigations
- Long-term antibiotic treatment may be useful
Complications
- Pathologic fracture
- Osteomyelitis
- Draining fistulae


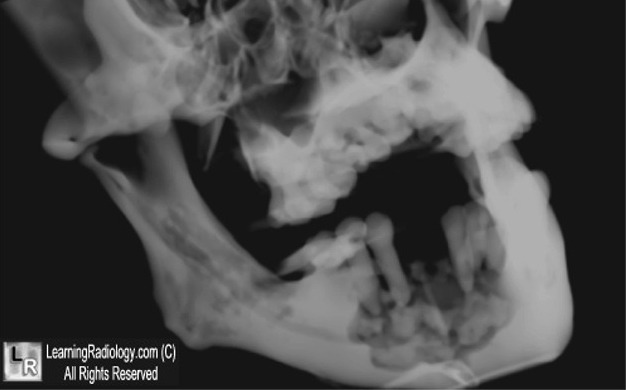
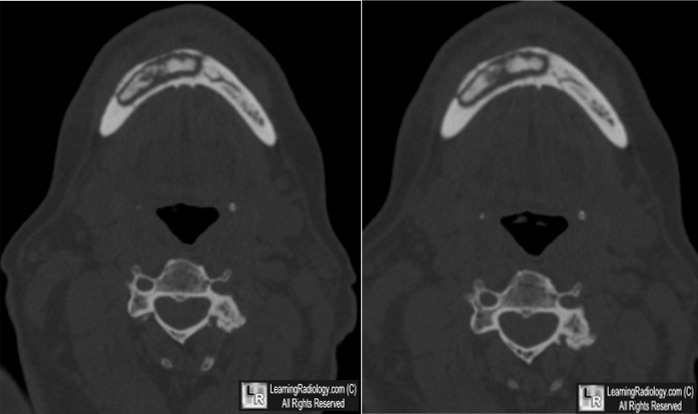
Bisphosphonate-related Osteonecrosis of the Jaw. Upper photo. Blue arrows point to a large lytic lesion in the right side of the mandible in a patient who had been on high-dose bisphosphonates for multiple myeloma. A tooth (white arrow) had recently been extracted. Lower photo: White arrows point to a lytic lesion in the right side of the mandible with a dense sequestrum within it.
For these same photos without the arrows, click here and here
For more information, click on the link if you see this icon 
Bisphosphonates and oral cavity avascular bone necrosis. J Clin Oncol 2003;21:4253-4
Bisphosphonate-related osteonecrosis of the jaw: the Florence experience. A Borgioli, M Duvina, L Brancato, C Viviani, ML Brandi, and P Tonelli. Clin Cases Miner Bone Metab. 2007 Jan–Apr; 4(1): 48–52.
eMedicine. Bisphosphonate-Related Osteonecrosis of the Jaw. RH Blanchaert, and CM Harris
|
|
|

{kind=link}
{kind=link}